Weight Loss and Disability: What No One Tells You About Finding Safe, Accessible Support
Why Standard Weight Loss Advice Fails Disabled People
Many weight loss plans overlook barriers disabled people face. Physical obstacles like limited mobility create problems. Social exclusion and inaccessible environments block access. They rarely centre disabled people’s insights when designing solutions.
Real Stories from Disabled People: Weight Loss and Accessibility
Firsthand Experiences from Disabled Communities
Reddit communities like r/ChronicIllness and r/Disabled are rich with real stories and advice from disabled people navigating weight loss:
- “Part of my weight loss mission included weekly gym visits with an exercise physiologist whose job is dealing with disabled people.”
- “Fwiw I lost 40lbs (20 of those were gained post-illness) and my condition has not seen much improvement. It definitely can help some folks but…”
These spaces are filled with requests for accessible support, adaptive strategies, and validation of the unique barriers faced.
Key Challenges: Quotes and Evidence
Reduced Mobility Limits Exercise and Calorie Burn
- “As I am disabled I can’t do normal exercises so I follow lots of hobbies to keep my mind, if not my body, active. This is a big disadvantage as I used to love walking, movement to music, ‘fun runs’, swimming, etc.”
- “I’m not able to do a lot of things that I used to be able to do. I can’t do a lot of walking. I can’t do a lot of lifting. So, I have to be cautious of everything I do now…”
Chronic Conditions Affect Energy, Pain, and Movement
- “Chronic illness often brings biochemical challenges that make weight loss difficult, such as slow metabolism, hormonal imbalances, systemic inflammation, gut issues, medication side effects, and emotional factors like depression, anxiety, and emotional and biochemical based food cravings.”
- “Chronic conditions can affect metabolism, energy levels, and dietary needs, making weight loss more challenging.”
Medications and Hormonal Shifts Can Stall Progress
- “I was put on steroids and this piled the weight on.”
- “Conditions like gut dysbiosis, poor carbohydrate metabolism, low digestive enzyme activity, and hormone imbalances (like insulin, cortisol, and thyroid dysfunction) can all interfere and make weight loss almost impossible.”
Scarcity of Accessible Facilities and Adaptive Equipment
- “Adults with mobility related disabilities (MRDs) face several barriers to participation in weight management. For example, the lack of affordable, accessible transportation represents a significant barrier for both attending on-site meetings required in traditional weight management programs, and for engaging in physical activity… confronted with inaccessible recreational facilities, lack of affordable and accessible fitness equipment, and poor infrastructure for physical activity (lack of sidewalks and curb cuts, narrow/damaged sidewalks etc.).” (BBC: Is it harder for disabled people to lose weight?)
Professionals with Disability Expertise Are Hard to Find
- “Part of my weight loss mission included weekly gym visits with an exercise physiologist whose job is dealing with disabled people.”
- “People with learning disabilities benefit from a multi-disciplinary and multi-component approach that takes an individualised approach.”
Stigma, Discrimination, and Lack of Social Support
- “Obesity stigma may be associated with increased difficulty of losing weight and medication non-adherence and people with obesity may exclude themselves from some exercise settings.”
- “I want a healthy lifestyle. But it’s often inaccessible to disabled people like me. Diet and exercise are especially challenging for disabled people.” (Vox: I’m obese and disabled. A healthy lifestyle is inaccessible to people like me)
Standard Weight Loss Advice Often Excludes Disabled People
- “Recommendations like ‘move more’ or ‘go to the gym’ assume a body free of pain, fatigue and mobility limits. This leaves many excluded.”
- “When I am confined to the wheelchair my weight remains stable or increases. If I walk my weight drops. I am determined not to sit in the wheelchair forever. When we go out anywhere I push it until I can walk no further, then sit in it.”
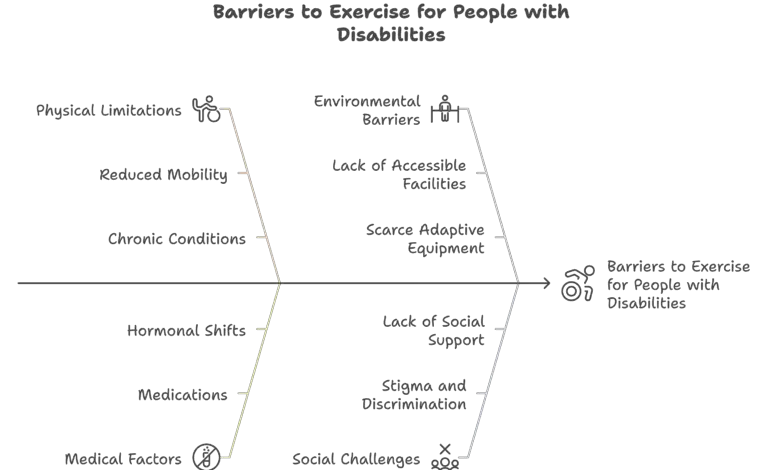
To sum up:
- Reduced mobility limits traditional exercise options and lowers calorie burn
- Chronic conditions affect energy, pain levels and movement
- Medications and hormonal shifts can stall progress
- Accessible facilities and adaptive equipment are scarce
- Professionals with disability expertise can be hard to find
- Stigma, discrimination and lack of social support discourage engagement
Disabled people encounter unique challenges that standard weight loss advice overlooks. Recommendations like “move more” or “go to the gym” assume a body free of pain, fatigue and mobility limits. This leaves many excluded.

Physical Barriers and Inaccessibility
Instructions to “exercise” often require standing or walking. This may be painful or impossible.
Gyms frequently lack ramps, accessible locker rooms and machines. These don’t adapt to wheelchairs or seated positions.
Public transport routes may not stop near fitness centres. Accessible taxis can be costly or scarce.
Inadequate Dietary Guidance
Calorie calculators do not account for altered metabolism. Conditions like spinal injury or muscle atrophy change needs.
Tasks such as chopping vegetables, lifting heavy cookware or opening jars can be too taxing. Someone with limited hand function struggles with these.
Program Design Gaps
Many weight loss plans centre around in-person group classes at fixed times. This ignores those who need remote or flexible options.
Few interventions include seated, aquatic or adaptive exercises. These should be tailored to varied mobility levels.
Social and Psychological Barriers
Being the only disabled person in a class can feel isolating. It draws unwanted attention.
Weight stigma, microaggressions and unsupported environments undermine confidence. They reduce motivation.
Medical Factors
Medications for chronic conditions can boost appetite and cause water retention. Steroids and certain antipsychotics do this.
Hormonal fluctuations from treatments or conditions may stall weight loss. This happens despite strict diet changes.
Complex Health Needs
People with coexisting health conditions may need more specialised dietary or activity plans. Standard advice doesn’t provide this.
Lack of Professional Knowledge and Training
Many providers aren’t equipped to adapt weight loss advice for disabled people. This leads to generic or inappropriate recommendations.
Few providers refer patients to accessible weight loss services. These are often scarce.
Healthcare Bias and Being Dismissed
Healthcare bias against disabled people can manifest through negative assumptions. Denial of care and dehumanising interactions happen. This causes substandard care, emotional distress and avoidable health disparities.
Disabled people often face assumptions about their competence and quality of life. This leads to withheld treatments and the belief that further care is futile.
The Realities of Being Dismissed
Conscious or unconscious bias against disabled people can lead to their concerns being ignored or minimised. Healthcare providers make assumptions about a person’s competence or quality of life. They may skip tests, withhold treatments or fail to explain options clearly. This erodes trust and can delay diagnoses, worsen health and discourage future care.
- Assumptions about fragility can result in withheld or inappropriate treatments
- Overlooking possible diagnoses can lead to preventable complications
- Dehumanising interactions cause emotional distress and loss of confidence in care
- Substandard treatment increases preventable hospital admissions and unmet needs
What Accessible Support Could Actually Look Like
Truly inclusive weight loss support adapts every aspect of a program. From design to delivery and environment, it meets diverse needs. This means offering flexible, personalised services in nutrition, exercise, digital tools and social settings.
Inclusive Program Design
- Adapted curriculum: Exercises and lessons modified for physical, sensory or intellectual differences
- Flexible delivery: A mix of group, one-on-one, remote and in-person sessions to suit varied schedules and mobility
- Personalised plans: Tailored calorie guidance, portion-controlled meals and alternative activities based on individual abilities
Accessible Physical Activity
- Adaptive fitness: Chair-based aerobics, resistance-band routines, aquatic therapy and adaptive sports
- Trained professionals: Coaches educated in disability inclusion to ensure safe, effective and enjoyable workouts
- Home and community options: Equipment and resources for home use, plus accessible facilities in local centres
Accessible Nutrition Support
- Meal prep made simple: Plans featuring microwave-friendly or ready-to-eat options, shopping tips and energy-saving kitchen hacks.
Meal Replacement Solutions for Accessible Weight LossFor many disabled people, the effort needed to shop for ingredients, chop vegetables, and cook a balanced meal can be a major barrier—especially when mobility restrictions, fatigue, or pain are part of daily life. On days when those barriers feel heavier, meal replacement shakes such as The Man Shake Australia can be a straightforward alternative. They offer consistent portion sizes, steady protein, and balanced nutrition without the time and energy that full meal prep demands.
These shakes aren’t a substitute for all whole foods, but they can slot into a routine as a practical tool for managing calorie intake. This can be especially helpful during flare-ups or busy periods when preparing a fresh, healthy meal from scratch simply isn’t realistic. For some, having a ready-to-drink option in the cupboard is less about dieting and more about removing one more obstacle from the day.
- Portion tools: Visual guides and pre-measured meals to ease portion control
- Dietitian access: Telehealth or in-person consultations with dietitians experienced in disability nutrition
Digital and Remote Support
Websites and apps compatible with screen readers and alternative input methods help people track progress. Self-monitoring tools for tracking progress, setting goals and connecting with peer support online work well.
Online support from coaches or peers can boost motivation. It builds accountability and eases isolation for disabled people.
Environmental and Social Support
- Accessible facilities: Gyms, pools and weight centres with ramps, wide doors and adaptive equipment, plus staff trained in disability inclusion
- Family and carer involvement: Educating families and carers ensures daily assistance aligns with health goals and decision-making support
- Community integration: Partnerships with local disability organisations and services help reduce stigma and strengthen inclusion
Inclusive Communication and Training
- Staff training: All staff should receive disability awareness education and learn to communicate clearly about participants’ needs
- Accessible materials: Provide resources in print, digital and visual formats that work with screen readers and alternative inputs
- Feedback channels: Invite disabled people to share barriers and suggestions so programs can continuously improve
Medication Options, Including Mounjaro
When mobility limits make traditional exercise impractical, weight-loss pens like Mounjaro can help manage weight without intense activity.
Effectiveness
Higher doses of Mounjaro have led to up to 22.5% weight reduction over 72 weeks in clinical trials.
How It Works
- Appetite regulation: Promotes fullness and reduces cravings
- Blood sugar control: Supports better glucose levels and may lower cardiovascular risk
Considerations for Disabled People
Once-weekly injections can be easier to manage than daily pills. This is especially true for those with dexterity or memory challenges. Medical supervision is essential to monitor side effects and adjust treatment.
Combining Medication with Other Supports
These medications can complement adapted nutrition plans, telehealth coaching and peer support. This creates a more inclusive weight loss strategy.
Safety Concerns
- Nausea, vomiting, diarrhoea, constipation or other digestive issues
- Rare but serious risks like pancreatitis, severe abdominal pain or kidney complications
- Requires close supervision by healthcare providers, especially for disabled people with complex health needs
Your Body, Your Choice
- Personal goals: Decide if, when and how to pursue weight loss, with support tailored to your priorities
- Informed consent: Accessible information about risks and benefits helps you choose what aligns with your values
- No one-size-fits-all: Reject standard plans that ignore individual abilities and preferences
- Respect over pressure: Avoid shame or guilt and foster a non-judgmental atmosphere
- Self-advocacy: Speak up about needs, request adaptations or opt out of interventions at any time
- Diverse outcomes: Support goals that prioritise quality of life, independence and self-esteem over weight loss alone
- Right to say no: You can decline any treatment or advice that doesn’t fit your goals
- Centre disabled voices: Involve disabled people in designing and leading programs to ensure respectful, accessible support
Conclusion
Weight loss advice must work for everyone. If advice ignores disability, it can stop us hearing important ideas.
It can spread unfair bias. Health workers can do three things:
- Make programs that include disabled people
- Offer medical options that suit each person’s needs
- Respect your right to choose
These steps help you stay healthy in your own way.